In any clinical setting, clear, concise, and structured communication is the cornerstone of effective patient care. For healthcare professionals navigating complex cases and collaborating across disciplines, a standardized method for documenting patient encounters is not just a convenience—it’s a necessity. This is precisely where a high-quality Soap Report Template becomes an indispensable tool, providing a logical framework to capture critical information efficiently and accurately. By organizing data into distinct categories, these templates streamline the documentation process, reduce the risk of errors, and ensure that every member of the care team has a clear understanding of the patient’s condition and treatment plan.
The SOAP note, an acronym for Subjective, Objective, Assessment, and Plan, is a widely adopted method for documentation in healthcare and other related fields. It was developed by Dr. Lawrence Weed in the 1960s as part of the problem-oriented medical record (POMR). The structure is designed to mirror the clinical reasoning process, starting with what the patient reports, followed by the provider’s objective findings, leading to a professional assessment, and culminating in a clear plan of action. This logical flow makes it an incredibly powerful format for both initial evaluations and follow-up visits.

Using a pre-designed template for SOAP reports offers significant advantages over free-form note-taking. It promotes consistency across all patient records within a practice, ensuring that vital information is never omitted. This standardization is crucial not only for patient safety and quality of care but also for legal documentation and billing purposes. For students and new practitioners, a template serves as a valuable learning aid, guiding them through the process of thorough data collection and clinical decision-making.
This article will serve as a comprehensive guide to understanding, utilizing, and customizing SOAP report templates. We will delve into the specific components of each of the four sections, explore the profound benefits of adopting a standardized template, and provide practical advice for implementing this system in various clinical specialties. Whether you are a seasoned physician, a physical therapist, a mental health counselor, or a student entering the medical field, mastering the use of a SOAP report template is a critical step toward elevating the quality and efficiency of your practice.
What is a SOAP Note? A Foundational Overview
A SOAP note is a structured method of documentation used by healthcare providers to record a patient’s visit. Its primary purpose is to organize information in a clear and universally understood format, facilitating communication among care team members and providing a chronological record of a patient’s medical journey. The acronym SOAP stands for the four distinct sections of the note, each serving a unique function in telling the patient’s story.
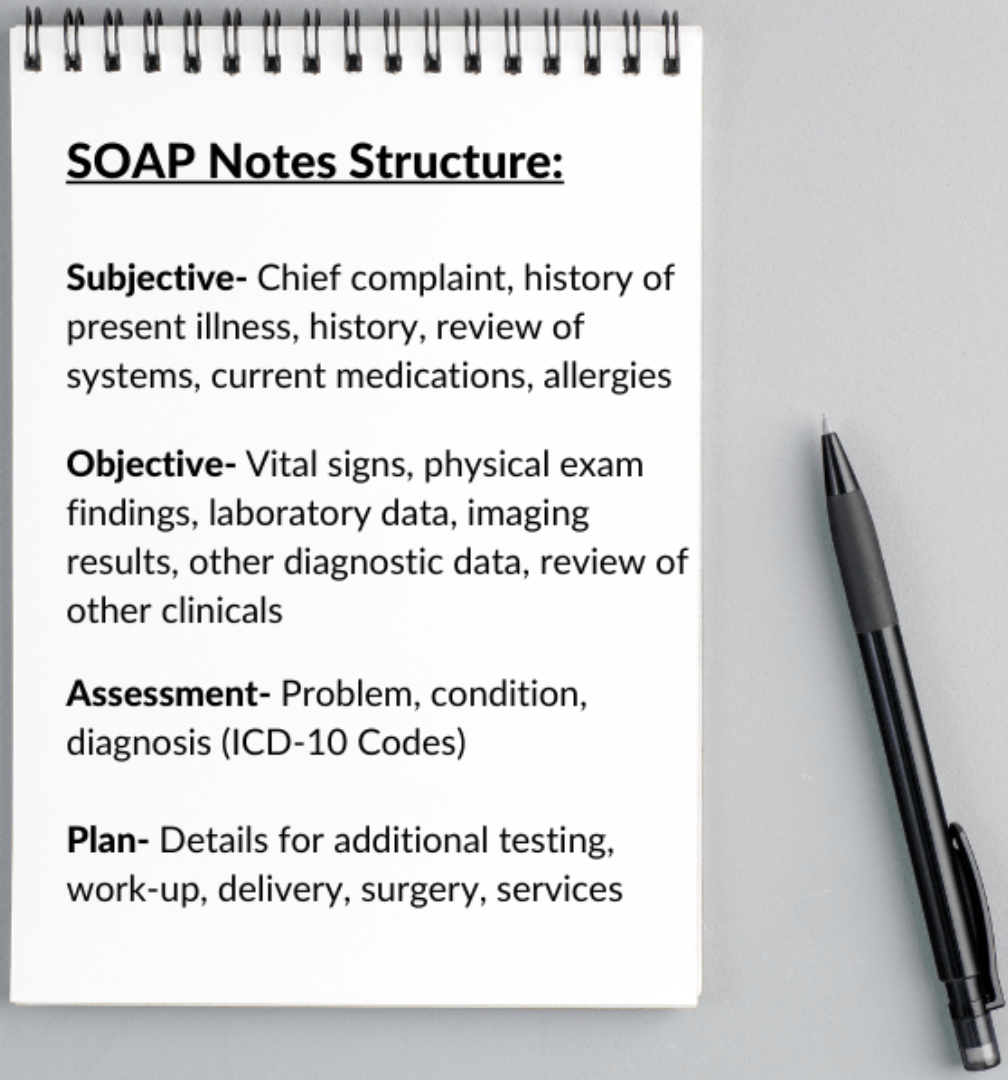
S – Subjective
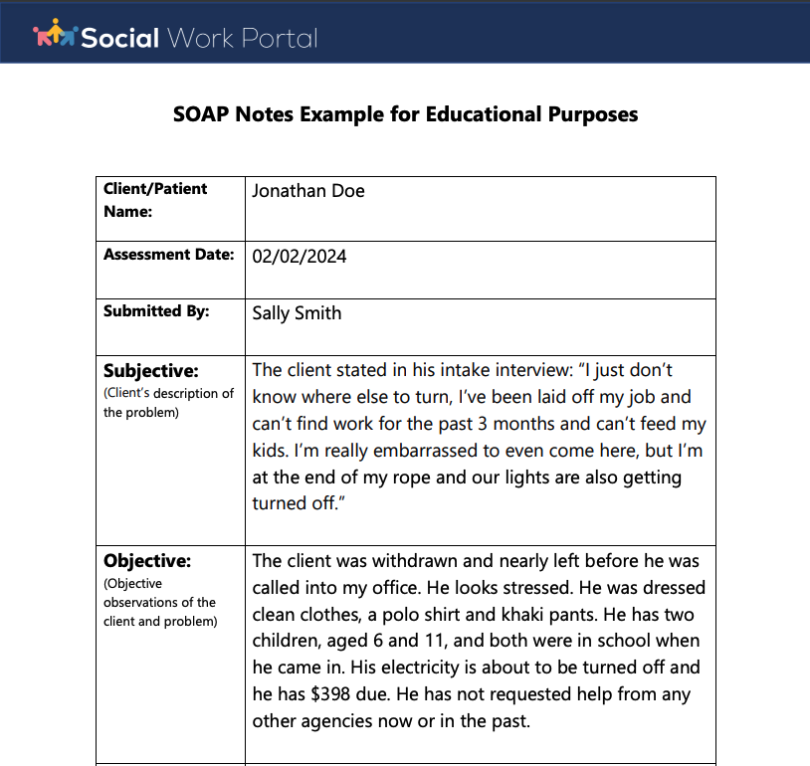
This is the first section of the report and it captures the patient’s personal account of their condition. It is “subjective” because it is based on the patient’s feelings, perceptions, and experiences. Information in this section is obtained through conversation and interviews with the patient or their caregiver. Key components include the Chief Complaint (CC), which is the primary reason for the visit, often stated in the patient’s own words (e.g., “I have a sharp pain in my lower back”). It also includes the History of Present Illness (HPI), a detailed narrative of the chief complaint, and the Review of Systems (ROS), a systematic questioning about different body systems. Past medical history, surgical history, family history, social history, current medications, and allergies are also documented here.

O – Objective
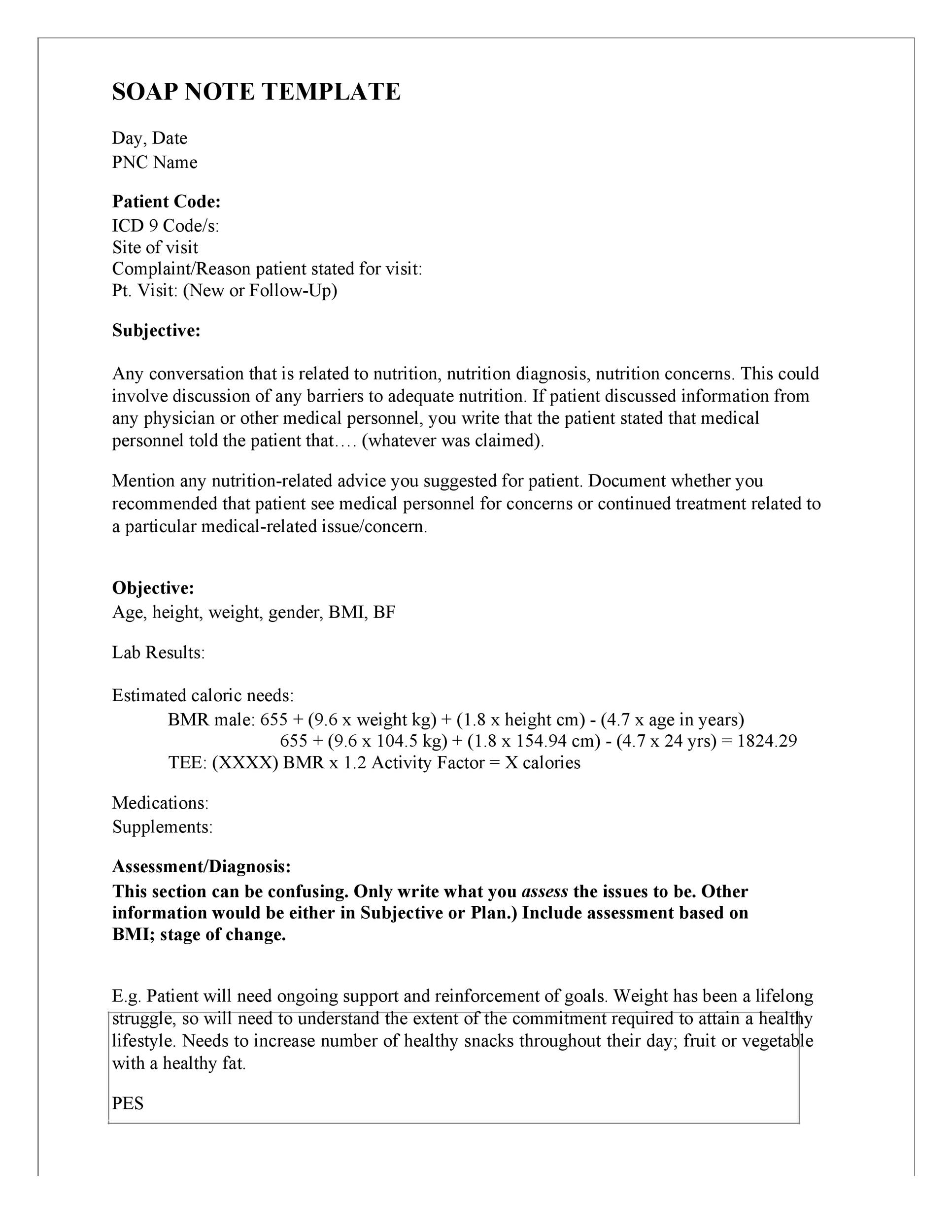
The objective section contains factual, measurable, and observable data gathered by the healthcare provider. This information should be unbiased and reproducible. It is the evidence that supports or refutes the subjective claims made by the patient. Common elements of the objective section include vital signs (blood pressure, heart rate, temperature, respiratory rate), findings from a physical examination, and the results of laboratory tests and other diagnostic imaging like X-rays or MRIs. For example, under the physical exam, a provider might note “tenderness to palpation over the lumbar spine” or “limited range of motion on forward flexion.”
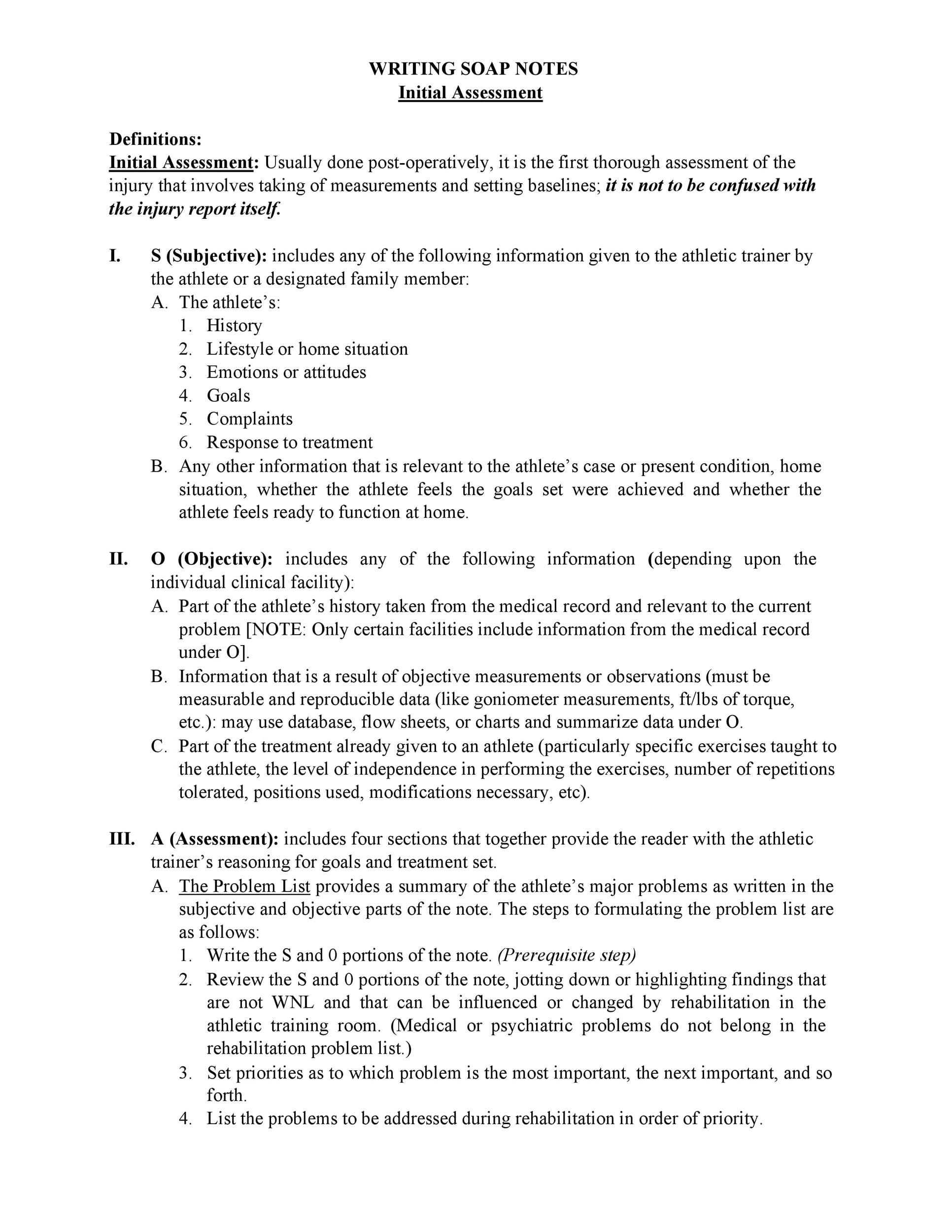
A – Assessment
In the assessment section, the healthcare provider synthesizes the subjective and objective information to arrive at a professional conclusion. This is the core of clinical reasoning. The assessment includes the primary diagnosis and, if applicable, a list of differential diagnoses—other possible conditions that could be causing the patient’s symptoms. For a patient with back pain, the assessment might be “1. Acute Lumbar Strain.” For more complex cases, it might involve a prioritized list of problems. This section directly links the patient’s story and the provider’s findings to a specific medical condition.
P – Plan
The final section outlines the course of action to address the patient’s condition as identified in the assessment. The plan should be specific, actionable, and comprehensive. It details what the healthcare provider will do, and what the patient is expected to do, to manage the problem. This can be broken down into several parts: diagnostic plans (e.g., “Order lumbar spine X-ray”), therapeutic plans (e.g., “Prescribe Ibuprofen 600mg every 8 hours as needed for pain”), patient education (e.g., “Discuss proper lifting techniques and provide handout on back-strengthening exercises”), and follow-up instructions (e.g., “Return to clinic in 2 weeks for re-evaluation”).
The Anatomy of a Comprehensive Soap Report Template
A well-designed template does more than just provide four blank sections labeled S, O, A, and P. It acts as a detailed checklist, guiding the user to capture all necessary information methodically. This ensures completeness and consistency, which is vital for high-quality care.

Basic Patient Information
Before diving into the SOAP structure, every template should begin with a section for essential patient identifiers. This prevents confusion and ensures the note is correctly filed in the patient’s chart. This area typically includes:
- Patient’s Full Name
- Date of Birth (DOB)
- Patient Identification Number or Medical Record Number (MRN)
- Date and Time of Visit
- Name and Title of the Provider
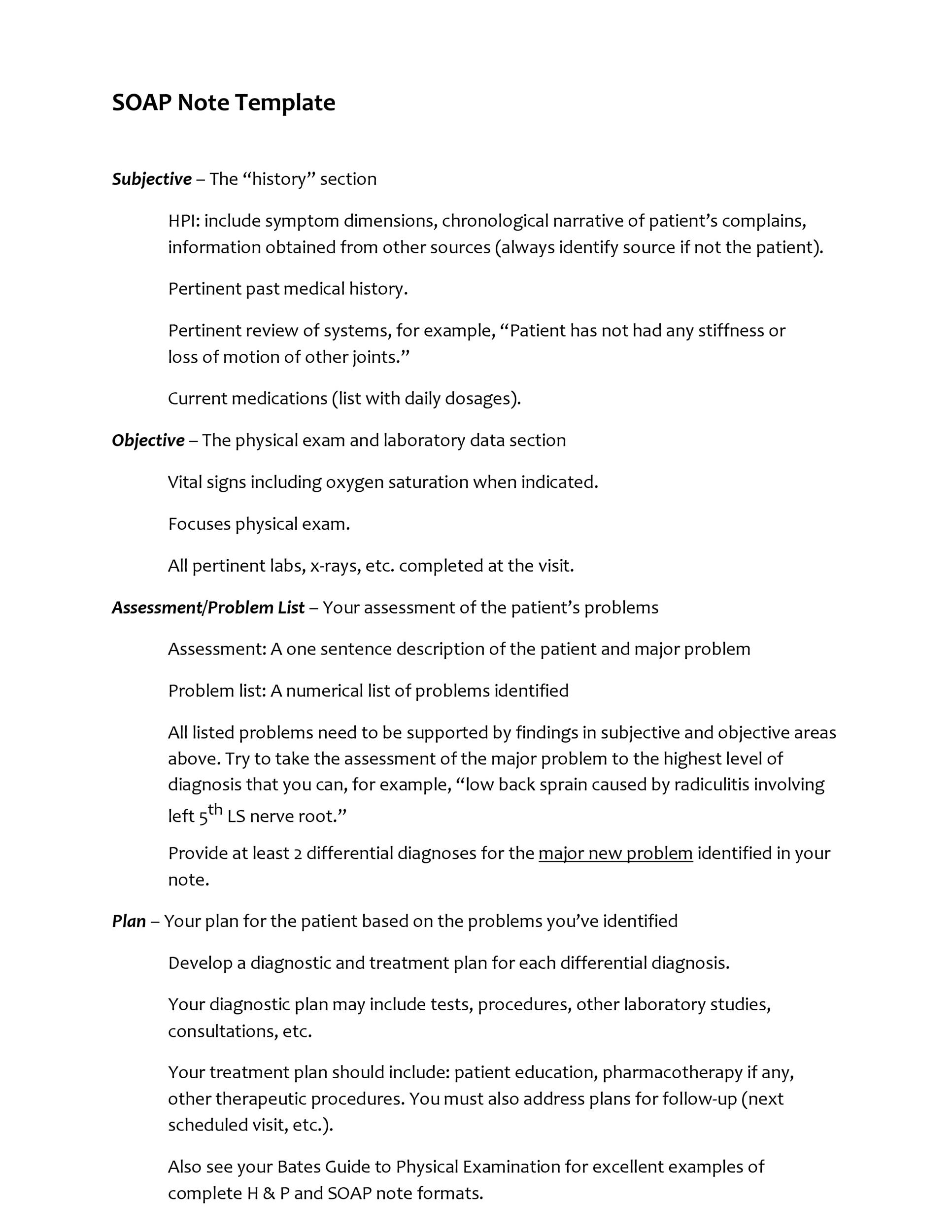
The “S” – Subjective Section
A robust template will break down the subjective section into clear prompts to ensure a thorough history is taken.

- Chief Complaint (CC): A single line to record the main reason for the visit in the patient’s own words.
- History of Present Illness (HPI): This is the most detailed part of the subjective section. A good template may use a mnemonic like OLDCARTS (Onset, Location, Duration, Character, Aggravating/Alleviating factors, Radiation, Timing, Severity) to prompt for a complete story of the illness.
- Past Medical History (PMH): A checklist or space for chronic illnesses, past surgeries, and major medical events.
- Medications: A list of current prescriptions, over-the-counter drugs, and supplements, including dosage and frequency.
- Allergies: A clear section for drug, food, and environmental allergies and the type of reaction.
- Review of Systems (ROS): Often a checklist format organized by body system (e.g., Constitutional, Cardiovascular, Respiratory, GI) to quickly screen for other associated symptoms.
- Social/Family History: Prompts for relevant information about lifestyle (smoking, alcohol use), occupation, and significant family medical history.
The “O” – Objective Section
This section of the template should be organized to present factual data logically.
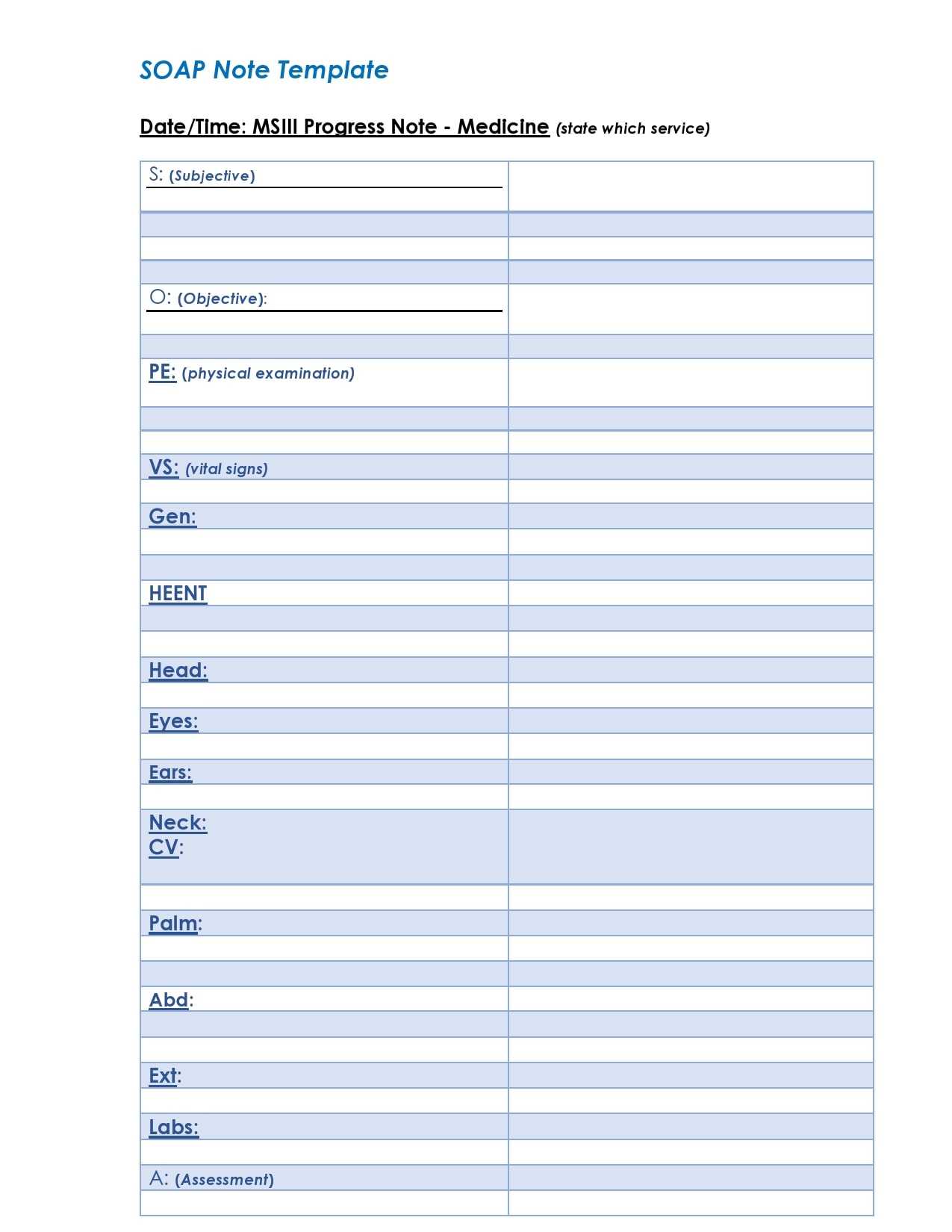
- Vital Signs: Designated fields for Temperature, Blood Pressure, Heart Rate, Respiratory Rate, and Oxygen Saturation.
- Physical Examination: This is often structured by body system. A template for a primary care physician will have sections for General Appearance, HEENT (Head, Eyes, Ears, Nose, Throat), Cardiovascular, Pulmonary, Abdominal, Musculoskeletal, Neurological, and Skin. This ensures a systematic and comprehensive exam is documented.
- Diagnostic Results: A dedicated area to list results from labs, imaging, or other tests that are available at the time of the visit.
The “A” – Assessment Section
The template should encourage a clear and prioritized list of diagnoses.
- Problem List/Diagnosis: Often a numbered list. The primary diagnosis should be listed first, followed by any secondary or chronic conditions addressed during the visit. For example: “1. Acute Pharyngitis. 2. Hypertension (chronic, stable).”
- Differential Diagnosis: A space to list alternative possibilities that are being considered, especially for new or undifferentiated problems.
The “P” – Plan Section
A quality template breaks the plan into distinct, actionable categories to ensure nothing is missed.

- Diagnostics: Any labs, imaging, or tests that are being ordered.
- Treatments/Therapeutics: New medications prescribed, procedures performed, or therapies initiated.
- Referrals: Any referrals being made to specialists.
- Patient Education: Key topics discussed with the patient, such as disease process, lifestyle modifications, or medication side effects.
- Follow-up: Specific instructions on when and why the patient should return or seek further care.
Why Use a Template? The Benefits of Standardization
While some practitioners may prefer the flexibility of a blank page, the benefits of adopting a standardized template for SOAP notes are overwhelming. It transforms documentation from a chore into a powerful clinical tool.
One of the most immediate benefits is efficiency and time-saving. A template with prompts and checklists significantly reduces the cognitive load on the provider, allowing them to focus on the patient rather than on remembering every documentation requirement. It minimizes the time spent typing or writing, which is a major factor in preventing provider burnout.

Consistency and clarity are also key advantages. When all providers in a group use the same format, it becomes incredibly easy for anyone to pick up a patient’s chart and quickly understand their history and current status. This uniformity is crucial for continuity of care, especially in team-based settings or during patient handoffs.

This leads directly to improved communication. A well-structured SOAP note is a universally understood language among healthcare professionals. A specialist reviewing a referral or a colleague covering a shift can immediately locate the assessment and plan without having to hunt through paragraphs of prose. This clarity reduces the potential for misinterpretation and medical errors.
Furthermore, a template acts as a safeguard to reduce errors of omission. By providing dedicated spaces and checklists for things like allergies, past medical history, and a review of systems, the template ensures that critical pieces of information are not accidentally overlooked during a busy clinic day. This structured approach creates a more thorough and legally defensible medical record, which is essential for both legal and billing compliance. Accurate and complete documentation is required to justify medical billing codes and to provide a robust defense in the event of a malpractice claim.

How to Effectively Use Your Soap Report Template
Having a great template is only half the battle; knowing how to use it effectively is what truly enhances patient care. Following best practices ensures that your documentation is not only complete but also clinically meaningful.
Be Concise but Thorough
Your notes should be a clear and accurate reflection of the patient encounter without being overly verbose. Use widely accepted medical abbreviations to save space and time, but avoid obscure or personal shorthand that others may not understand. The goal is to provide enough detail for another provider to fully grasp the patient’s situation, but not so much that the key information gets lost in a wall of text.
Maintain Objectivity
It is crucial to distinguish between subjective and objective information. In the ‘S’ section, document the patient’s story. Using direct quotes can be powerful (e.g., Patient states, “the pain feels like a hot poker”). In the ‘O’ section, stick strictly to the facts. Record what you observed, measured, or palpated. Avoid including opinions or interpretations in this section; that belongs in the Assessment.
Link Assessment to Evidence
The ‘A’ section should be a logical conclusion based on the evidence presented in the ‘S’ and ‘O’ sections. Your assessment is your professional judgment, and it should be clearly justified by the data you’ve collected. If you are diagnosing a urinary tract infection, the ‘S’ section should mention symptoms like dysuria and frequency, and the ‘O’ section should include findings like suprapubic tenderness or urinalysis results.
Create Actionable Plans
The ‘P’ section is your roadmap for patient management. Make it specific and clear. Instead of writing “follow up as needed,” write “follow up in 1 week to review lab results and assess response to treatment.” For prescriptions, include the medication, dose, route, and frequency. A well-defined plan ensures that both the patient and the rest of the healthcare team know exactly what the next steps are.
Regular Review and Updates
Your documentation needs can change over time. Periodically review your template to see if it is still serving your needs effectively. Are there fields you never use? Is there information you consistently have to add in the margins? Don’t be afraid to customize and update your template to better fit your personal workflow, specialty requirements, or new institutional guidelines.
Types of Soap Report Templates for Different Specialties
While the core SOAP framework is universal, the specific content and focus of a template can vary significantly depending on the clinical specialty. A one-size-fits-all approach is rarely optimal.
General Medicine / Primary Care
Templates for primary care are typically broad and comprehensive, designed to handle a wide variety of acute and chronic conditions. They often feature an extensive Review of Systems checklist and prompts for health maintenance topics like vaccinations and cancer screenings. The plan section may include a diverse range of interventions, from medication management to lifestyle counseling.
Physical or Occupational Therapy
A therapy-based Soap Report Template places a strong emphasis on function. The Subjective section will focus on the patient’s reported pain levels, functional limitations, and progress toward their goals. The Objective section is heavily focused on measurable data like range of motion, strength testing, balance assessments, and performance on specific functional tasks. The Assessment details progress, and the Plan outlines the specific exercises, modalities, and interventions for the next session.
Mental Health Counseling
In mental health, the template is tailored to psychological and emotional assessment. The Subjective section is often the most detailed, capturing the client’s emotional state, recent life events, and self-reported symptoms. The Objective section includes a Mental Status Exam (MSE), observing appearance, mood, affect, and thought processes. The Assessment involves a diagnostic impression based on DSM criteria, and the Plan details therapeutic interventions, coping strategies, and goals for the next session.
Nursing
Nursing SOAP notes often focus on monitoring patient responses and managing the care plan. The Subjective part might include the patient’s reported pain level or concerns. The Objective section contains vital signs, wound appearance, or intake/output measurements. The Assessment evaluates the patient’s response to interventions (e.g., “Pain decreased following medication”), and the Plan outlines ongoing nursing care, such as patient education or continued monitoring.
Veterinary Medicine
The SOAP structure is also a standard in veterinary medicine. The Subjective section is unique as it captures the owner’s observations of the animal’s behavior, appetite, and symptoms. The Objective section includes the veterinarian’s physical exam findings and diagnostic results. The Assessment and Plan follow the same principles as in human medicine, leading to a diagnosis and a treatment strategy for the animal patient.
Conclusion
The SOAP note format is more than just a documentation standard; it is a structured framework for clinical thinking that has stood the test of time. By breaking down a patient encounter into Subjective, Objective, Assessment, and Plan, it ensures a logical and comprehensive approach to patient care. Implementing a Soap Report Template elevates this process by introducing efficiency, consistency, and a crucial safety net against errors of omission.
For healthcare providers across all disciplines, a well-designed template saves valuable time, enhances communication with colleagues, and creates a clear, defensible legal record. It transforms the often-daunting task of documentation into a streamlined workflow, allowing clinicians to dedicate more of their energy to their primary mission: providing excellent patient care.
Whether you choose a pre-made template from your EHR system, download one from a professional organization, or customize your own to fit the unique needs of your practice, embracing this tool is a powerful step toward operational excellence. The clarity and structure it provides are fundamental to improving patient outcomes and fostering a collaborative and safe healthcare environment.
]]>


